It can also be called Diastasis recti of the abdominal muscles (DRAM) or tummy gap. It is the widening and thinning of a small connective tissue which runs down our midlines, dividing our six pack muscle into two halves. This connective tissue is called the linea alba and it runs all the way from the bottom of our sternum to our pubic bone. As the tissue widens, the two halves of the six pack muscle move further apart, and this is where the term ‘tummy muscle separation’ comes from.
PGP is common, affecting 1 in 5 pregnant women, and can affect your mobility and quality of life.
PGP can be mild to severe but is treatable at any stage in pregnancy and the sooner it is treated, the more likely you are to feel better. It is more common later in pregnancy.
Recent evidence shows that sexual health issues are very common after birth, with 61% of women reporting problems with pain during sex at three months postpartum, and 20% at twelve months postpartum. This simply means you are far from alone if postpartum sex is less desirable than before pregnancy.
Regardless of how you give birth, your pelvic floor supports your uterus and baby throughout your pregnancy, and pelvic pain after c-section, particularly during sex, is very common too.
The causes of pain during sex can vary and must be carefully evaluated to be treated appropriately. We know that the postpartum period is a very delicate time for women, as they face a series of changes, a lot of tiredness, and even postpartum depression. All of this can negatively impact your sex life.
The main factors related to the appearance of pain during sexual intercourse are linked to the following:
Hypertonicity of the pelvic floor/ difficulty relaxing pelvic floor: Sometimes birth (vaginal or c-section) can unmask latent trigger or tender points in the pelvic floor. This can make pain with penetrative or deep intercourse very painful.
presence of episiotomy;
vaginal lacerations;
breast-feeding;
pain during intercourse during pregnancy;
pain during sexual intercourse prior to pregnancy;
endometriosis;
depression;
image disturbances;
stress;
In addition, one of the frequent changes in postpartum women who breastfeed is vaginal dryness, which can only be noticed a little after childbirth (when sex life can resume), due to this pause period and hormonal changes. An increase in the hormone prolactin, which is responsible for milk production, very important in breastfeeding, will cause a decrease in circulating estrogen levels, responsible for vaginal lubrication.
That is why we will usually recommend the use of lots of lube for sex during this period!
There are other few things you can do to prevent or minimize pain during sex in the postpartum period.
First of all, see a pelvic floor physical therapist for a postpartum assessment to address your concerns.
They can be very helpful in checking your pelvic floor in finding the driver to why you may be experiencing dyspareunia in the first place.
You can also take part in quite a lot of foreplay and try different positions.
While some pain during postpartum sex can be common at first, it does not have to become chronic. If you’re experiencing painful sex after birth, seek help!
Coccydynia is nothing more than pain and discomfort located in the caudal portion of the spine (coccyx).
Coccygodynia is more commonly reported in females, due to anatomical issues of the pelvis and can be the result of trauma, repetitive injuries, postpartum, local tumors, degeneration or idiopathic nature (without known cause).
What are the causes of coccydynia?
The main cause of coccydynia is trauma, especially falling on your bottom, leading to a fracture of the coccyx, it can also be secondary to sitting for long periods on a hard surface.
It is not uncommon, however, when investigating cases of pain in the coccyx, to come across signs of instability in the coccyx region, such as hypermobility of the coccyx, which could also be another cause of pain.
Treatment
The treatment of coccydynia is most often conservative, without surgery. Decreasing the load/pressure from the coccyx using orthopedic pillows and avoiding sitting positions for too long are usually very effective measures.
In addition, analgesics and anti-inflammatories, as well as physiotherapy aimed at analgesia, coccyx manipulation techniques, relaxation and strengthening of the pelvic floor muscles.
Because there are numerous pelvic floor muscles that attach directly to the tailbone as well as pelvic joints around the tailbone, pelvic floor physiotherapy is very effective for this type of pain!
Some other tips:
Manage your constipation and avoid hard stools, which can aggravate the tailbone
Play with ice or heat and see if either helps you. If you use either one, limit it to ten minutes.
In cases that do not respond to these clinical measures, minimally invasive techniques such as local infiltrations with corticosteroids and anesthetics usually relieve symptoms well and are very resolving.
Have you ever heard about women who leak just a bit of urine when lifting weights at the gym? Or perhaps you have a friend who complains of small leakage or pain when going for a run? Or maybe when you exercise you may feel an intense pressure down there?
Technically, you’re not “in menopause” until you’ve gone a full year without a period. At that point, your ovaries are considered to be on a permanent vacation and you can no longer get pregnant. Perimenopause refers to the stage beforehand — when your ovaries are winding down. This period can be from 2 to 10 years before menopause during which changes in progesterone, estrogen, and testosterone hormone levels occur. The average age for menopause in New Zealand is 51.5 years but it can occur anytime between the ages of 42 and 56.
Endometriosis is a disease characterized by the presence of endometrium outside the uterus. The endometrium is the layer that lines the uterine cavity internally and is renewed monthly by shedding during the menstrual flow. In some situations this tissue, instead of being eliminated, returns through the tubes, and reaches the pelvic and abdominal cavity, generating endometriosis.
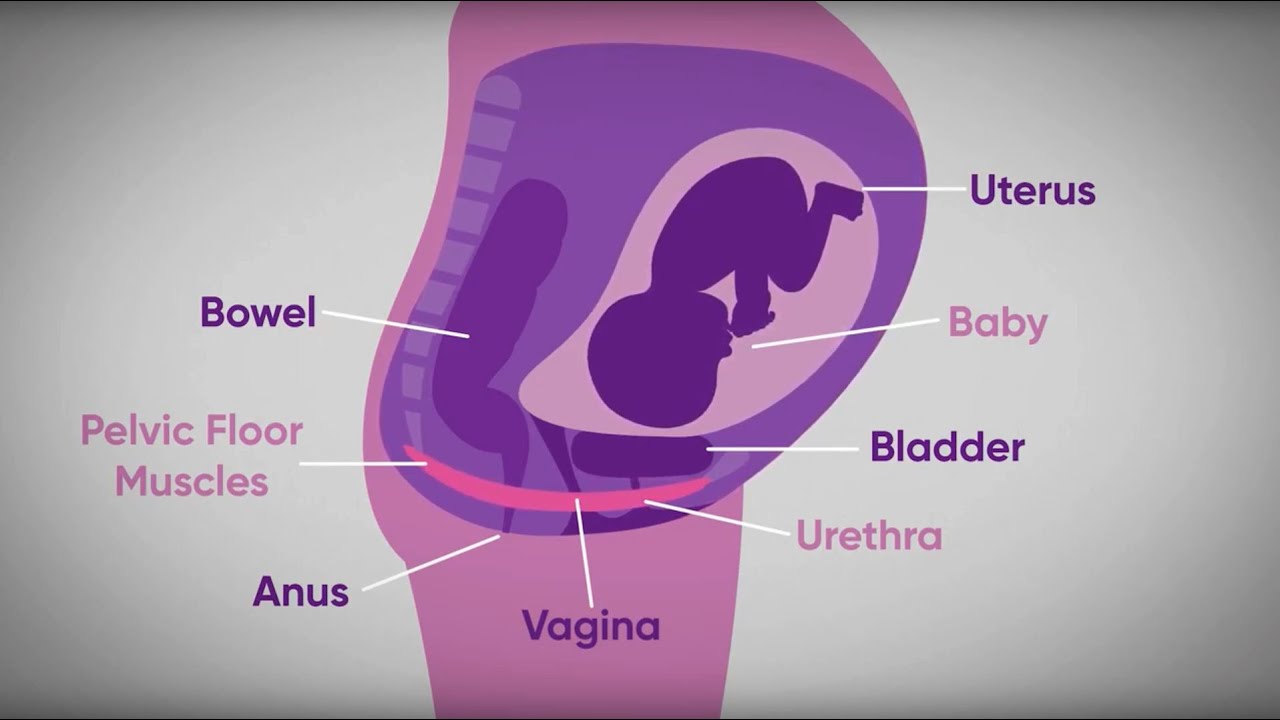
The levator ani muscle serves two major functions in the female body: supporting the vagina and pelvic organs and maintaining urinary and bowel continence. As a woman enters her third trimester and prepares for birth, these muscles become strained to support the baby’s growth and delivery.
You may even feel the need to use enemas, suppositories, or laxatives in order to maintain regular bowel movements.
What causes constipation?
Poor eating habits (for example, too much junk food, too much caffeine, irregular eating times)
Diet lacking in fiber and/or fluids
Lack of exercise
Some medications (including pain medications, tranquilizers, psychiatric medications, diuretics, iron supplements, calcium supplements, and aluminum containing antacids)
Stress
Pregnancy
Travel
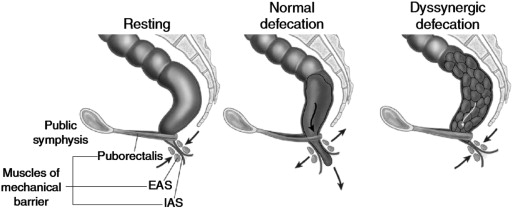
Problems with the function of the pelvic floor muscles. The muscles may not relax appropriately when trying to pass stool, making it difficult and sometimes painful to have a bowel movement.
As many as 50 percent of people with chronic constipation have pelvic floor dysfunction (PFD) — impaired relaxation and coordination of pelvic floor and abdominal muscles during evacuation.
Because slow transit constipation and functional constipation can overlap with pelvic floor issues, some patients may also present with other signs and symptoms, such as a long time between bowel movements and abdominal pain.
Treating constipation
Increase your fiber – Fiber helps general bowel health by bulking and softening stool which makes it easier to pass.
Allow yourself time after meals – allow time for the body’s natural emptying reflex. This reflex occurs approximately 30 minutes after eating a meal or drinking a hot beverage and is the body’s automatic mechanism to move stool. This usually happens in the mornings.
Proper position on the toilet – To allow for your pelvic floor muscles to relax as much as possible, it is helpful to properly position yourself (sit) on the toilet. Be sure your knees are positioned higher than your hips, use a foot stool if necessary.
See a Pelvic Floor Physiotherapist – Patients may meet individually with a specialist Pelvic Floor Physio who can provide a focused session on bowel management techniques. We can then begin retraining the pelvic floor muscles with biofeedback. Based on the principle of operant conditioning, biofeedback provides auditory and visual feedback to help retrain the pelvic floor and relax the anal sphincter.